Cervical spine trauma
Disclaimer
These guidelines have been produced to guide clinical decision making for the medical, nursing and allied health staff of Perth Children’s Hospital. They are not strict protocols, and they do not replace the judgement of a senior clinician. Clinical common-sense should be applied at all times. These clinical guidelines should never be relied on as a substitute for proper assessment with respect to the particular circumstances of each case and the needs of each patient. Clinicians should also consider the local skill level available and their local area policies before following any guideline.
Read the full CAHS clinical disclaimer
|
Aim
To guide staff with the assessment and management of cervical spine (C-spine) trauma.
Key points
- Cervical spine injury (CSI) should be suspected in all children with serious trauma, in particular in those with severe head injury.
- Australian and New Zealand Committee on Resuscitation (ANZCOR), International Liaison Committee on Resuscitation (ILCOR) and the State Spinal Cord Injury Service no longer recommend rigid cervical collar use in initial cervical spine immobilisation.
- Senior clinicians must assist in the assessment of children with suspected cervical spine injury to facilitate early removal of cervical spine immobilisation where appropriate and to limit exposure to radiation with imaging.
- The majority of paediatric trauma patients will not require neck imaging.
Background
- Suspected neck injuries are a common presentation to the emergency department, however, significant cervical spine injury following blunt trauma is uncommon occurring in only approximately 1% of all paediatric blunt trauma2.
- Children <8 years are more prone to sustaining high injuries (C1-C3) due to anatomical differences when compared to older children.
- Children >8 years have similar injury patterns to those seen in adults2.
Cervical spine assessment and identification of cervical spine injury is difficult. There are two validated clinical decision rule (CDR) for use in paediatrics: The Paediatric Emergency Care Applied Research Network (PECARN) prediction rule for cervical spine imaging of children2 and the Pediatric Cervical Spine Injury Following Blunt Trauma in Children Younger Than 3 Years (PEDSPINE II Study).3
Risk factors for cervical spine injury in children:4,5
- High-risk motor vehicle accident (MVA) (head-on collision, rollover, ejected from the vehicle, death in the same accident, high speed > 88 km/hr).
- Diving injury.
- Predisposing condition (e.g., trisomy 21, osteogenesis imperfecta, achondroplasia, other rheumatological, genetic or metabolic conditions or previous spinal surgery).
- Decreased neck range of motion.
Examination
Primary Survey
ABCDE as per APLS recommendations (see
Trauma - Serious injury), specific considerations in blunt neck trauma:
Airway:
Maintain airway precautions while maintaining inline cervical spine stabilisation.
Breathing / Circulation:
- Assess for any abnormalities with the patient’s breathing or circulation. In a multiple trauma or associated abdominal or chest trauma, consider eFAST (Extended Focused Assessment using Sonography in Trauma).
- In refractory hypotension consider spinal shock.
Disability:
- Assess Glasgow Coma Score (GCS) / Alert, responsive to Voice, responsive to Pain, or Unresponsive (AVPU) (including effect of sedative drugs / alcohol).
- Assess focal neurological deficit during primary survey (paraesthesia, numbness or weakness).
Environment/Exposure:
- Log roll (if not executed prior).
- Assess for substantial head or torso injury.
- Provide simple analgesia +/- opioids.
- SAMPLE history (Signs/Symptoms, Allergies, Medications, Past medical history, Last oral intake, and Events), including:
- High risk mechanism of injury:
- High risk MVA as above.
- Axial load to the head (trampoline, diving, fall from height).
- Substantial torso injury.
- Persisting symptoms of neck pain, paraesthesia or weakness.
Predisposing factors for cervical spine injury as above
Secondary Survey
If no risk factors were identified in the primary survey, the C-Spine can be clinically assessed during secondary survey:
- Consider detailed neurological exam as per ASIA if suspicious for neurological deficit, if normal proceed to clinical c-spine examination.
Clinical C-Spine examination6
During secondary survey if patient stable in primary survey.
- Palpate for tenderness along spinous processes from nuchal ridge to first thoracic vertebrae.
- Palpate lateral to the midline on right and left sides.
- If no significant tenderness and no abnormal neurology, assess active range of lateral rotation to 90 degrees and range of flexion and extension (chin to chest and look up) – stop if the child develops significant pain or neurological deficit.
- C-spine can be clinically cleared if no tenderness, no significant pain on movement and no red flags present.
- Once the C-Spine is clinically cleared the responsible medical practitioner must document this on the patient’s medical record.
Investigations
Based on the above-mentioned clinical criteria, careful consideration should be given whether a patient needs imaging of their spine, and which modality should be used.
- Plain radiographs present a significant lower exposure to radiation (+/- factor 10) than Computed Tomography (CT) scans and should be the investigation of choice for all patients without high-risk features of a fracture of their C-Spine. However, they have a slightly reduced sensitivity (<90%).7
- If X-ray does not show a fracture and there is ongoing concern regarding pain or reduced GCS, discuss with ED consultant and/or orthopaedic team regarding further imaging and management.
- A CT scan should be obtained in all unconscious patients (GCS<8, AVPU<V) and in those with traumatic respiratory failure, shock and abnormal focal neurological exam.
- Consider CT if another regional CT is indicated (especially head).
- Refer to orthopaedics team urgently if imaging shows a C-spine injury.
The following PECARN can be used to assist clinical decision for imaging:
PECARN high-risk features (12.1% risk of CSI) - consider CT
- GCS 3-8 or AVPU = U
- Abnormal airway/breathing/circulation
- Focal neurological deficit
PECARN intermediate-risk features (2.8% risk of CSI) - consider plain X-ray
Altered mental status (GCS 9-14 or AVPU = V/P)
- Midline neck pain or tenderness
- Substantial head or torso injury
None of the above risk features (0.2% risk of CSI)
Consider clinical clearance
Cervical Spinal Trauma Flowchart
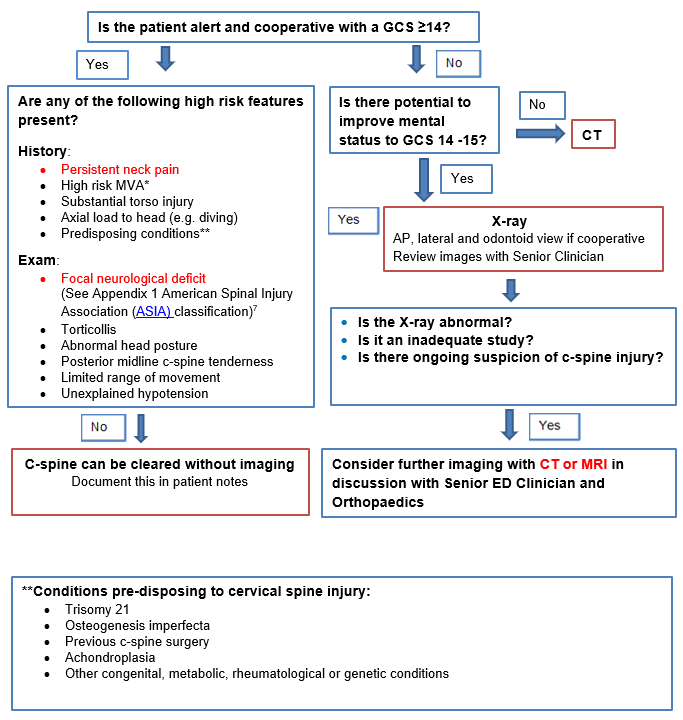
Image interpretation
There is no after hours X-ray reporting service from medical imaging at PCH.
ED doctors are responsible for timely X-ray interpretation. Discuss with ED consultant if any concern.
Use the C-Spine X-Ray pocket card for guidance.
Management
- Immobilisation and spinal precautions should be considered for all children with suspected cervical spine injury.
- Thoracic elevation device (TED) (eg. aeroplane pillow) should be considered in children younger than 8 years age to place the cervical spine in a neutral position if considered high risk for cervical spine injury or documented cervical spine injury. A TED (aeroplane pillow) is available from ward 1B at PCH.
- Head blocks or towel bollards can be used as a reminder for the patient to limit head movement.
- Avoid attempts to restrict spontaneous movement in an uncooperative child.
- Do not use Stifneck® type (hard) collars prior to imaging, if placed on child by external hospital or ambulance, remove while maintaining manual in-line stabilisation as soon as possible.
- Place a soft or semi rigid collar (e.g., Aspen) in the unconscious child.
- If C-spine injury cannot be excluded, place the patient in soft or semi rigid collar and discuss with orthopaedics.
- C-spine injury identified on imaging – immobilise and manage as per orthopaedics.
Nursing
- Complete and record a full set of observations on the age-appropriate Observation and Response Tool, add additional information on the Clinical Comments chart.
- Complete a full set of neurological observations if clinically indicated.
- Minimum hourly observations whilst in ED.
- Undertake regular pressure area care whilst in ED.
- Monitor for adequate urine output and assess for signs of urinary retention.
Patient Transfers
When transferring a patient from the ED trolley to the ward bed:
- Receiving ward staff will assume control of the patient’s head prior to the transfer / log roll.
- The transfer / log roll will be coordinated by the staff member in control of the patient’s head.
- ED staff will assist with the transfer / log roll as required.
- Specific requirements regarding bed tilt or break must be documented by the admitting team.
References
- Mohseni S, Talving P, Branco BC, Chan LS, Lustenberger T, Inaba K, et al. Effect of age on cervical spine injury in pediatric population: a National Trauma Data Bank review. J Pediatr Surg. 2011;46(9):1771-6.
- Leonard JC, Harding M, Cook LJ, Leonard JR, Adelgais KM, Ahmad FA, et al. PECARN prediction rule for cervical spine imaging of children presenting to the emergency department with blunt trauma: a multicentre prospective observational study. Lancet Child Adolesc Health. 2024;8(7):482-90.
- Luckhurst CM, Wiberg HM, Brown RL, Bruch SW, Chandler NM, Danielson PD, et al. Pediatric Cervical Spine Injury Following Blunt Trauma in Children Younger Than 3 Years: The PEDSPINE II Study. JAMA Surg. 2023;158(11):1126-32.
- Leonard JC, Kuppermann N, Olsen C, Babcock-Cimpello L, Brown K, Mahajan P, et al. Factors associated with cervical spine injury in children after blunt trauma. Ann Emerg Med. 2011;58(2):145-55.
- Tavender E, Eapen N, Wang J, Rausa VC, Babl FE, Phillips N. Triage tools for detecting cervical spine injury in paediatric trauma patients. Cochrane Database Syst Rev. 2024;3(3):Cd011686.
- Herman MJ, Brown KO, Sponseller PD, Phillips JH, Petrucelli PM, Parikh DJ, et al. Pediatric Cervical Spine Clearance: A Consensus Statement and Algorithm from the Pediatric Cervical Spine Clearance Working Group. J Bone Joint Surg Am. 2019;101(1):e1.
- Hopper SM, McKenna S, Williams A, Phillips N, Babl FE. Clinical clearance and imaging for possible cervical spine injury in children in the emergency department: A retrospective cohort study. Emerg Med Australas. 2020;32(1):93-9.
| Endorsed by: |
Nurse Co-director, Surgical Services |
Date: |
May 2026 |
This document can be made available in alternative formats on request for a person with a disability.