Foreign body - Ear
Disclaimer
These guidelines have been produced to guide clinical decision making for the medical, nursing and allied health staff of Perth Children’s Hospital. They are not strict protocols, and they do not replace the judgement of a senior clinician. Clinical common-sense should be applied at all times. These clinical guidelines should never be relied on as a substitute for proper assessment with respect to the particular circumstances of each case and the needs of each patient. Clinicians should also consider the local skill level available and their local area policies before following any guideline.
Read the full PCH Emergency Department disclaimer.
|
Aim
To guide PCH ED staff with the assessment and management of foreign bodies in the ear.
Background
- Foreign bodies (FB) in the external auditory canal in children are a common presentation to ED.
- It is more common in children less than 7 years or in older children with intellectual impairment.
- Most patients present soon after insertion due to distress, but occasionally may be delayed for days when the asymptomatic child divulges the history or may be discovered incidentally on routine ear examination.
- Removal of foreign bodies from the lateral third of the ear canal is much easier than deeper objects that may require ENT expertise +/- general anaesthesia for safe removal.
Key points
Types of foreign bodies
- A large variety of objects may be implicated. These include beads, plastic toys, vegetation, food, insects, pencils, crayons, cotton buds, paper, and putty.
- The most serious retained FB is the button battery that can cause mucosal damage and necrosis.
- A live insect as the FB is an ENT emergency (insect movement can cause severe distress) and the insect will need to be killed safely and quickly prior to its removal.
- Options in this case include instilling water or olive oil into the canal and shining a light on the ear.
- The insect will either “swim” to surface or drown. The dead carcass can be removed in a non-urgent manner.
- Sharp objects may cause canal and/or tympanic membrane trauma and these usually require ENT referral.
Factors influencing successful removal
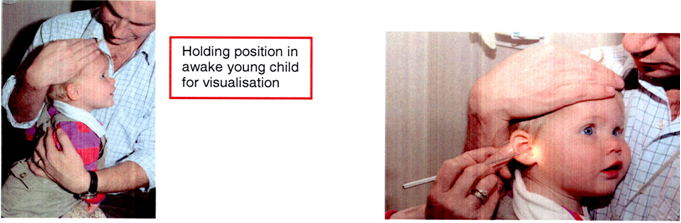
- Immobilisation and co-operation of patient
- Size and shape of FB
- Ability to visualise FB
- Repeated attempts at removal (the first attempt is usually the best chance in a young child)
- Available equipment
- Experience and skill of operator.
Assessment
Assessment is the key to determining the most suited technique of removal.
History
- If event is not witnessed, the child may present with irritation, pain, sensation of a foreign body or loss of hearing
- Examination
- Usually easily visualised by otoscopy or with a headlight
- Examination requires a still child and a good light source.
Management
- Removal options will depend on the type of object and its location in the canal
- The best suited technique for the particular object and location, will increase the success rate
- Ensure good lighting preferably with a headlight, so that two free hands can be used: for traction on ear with one hand and removal of the object with the other hand
- A cooperative or clinically held patient (by an assistant) is necessary to provide optimum conditions for removal. See Clinical Holding fact sheet (internal WA Health only).
- Consider sedation techniques. Consult Oral Conscious Sedation - Clinical Practice Manual (internal WA Health only) below and Ketamine sedation.
First choice
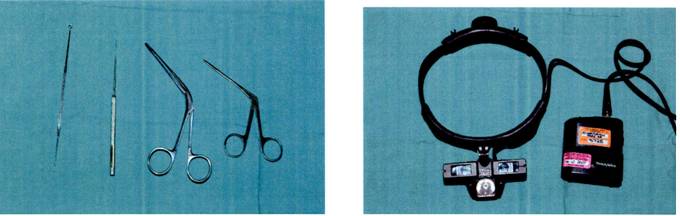
- Is normally under direct vision with surgical instruments such as an ear probe, alligator forceps or hook
- In general the probe or hook should be guided along the canal wall past the object and then used to pull the FB out from behind.
Alternative techniques
- Suction requires a smooth spherical object and can be successful provided a good seal is obtained between the end of the suction catheter and object
- Removal under a general anaesthetic by an ENT surgeon is indicated if simple techniques fail in the ED (can be arranged as an elective procedure on discussion with the ENT registrar).
Indications for ENT Team consultation
- Failure to remove object
- Evidence of trauma
- Button battery foreign body
- Penetrating foreign body.
Bibliography
- Isaacson GC, Aderonke O (2014) Diagnosis and Management of Foreign Bodies of the Outer Ear. UpToDate.
| Endorsed by: |
Co-Director Medical Services |
Date: |
Aug 2021 |
This document can be made available in alternative formats on request for a person with a disability.